Guideline-aware safeguards
Safety boundaries are designed around recognised clinical review expectations without publishing internal logic.
OralPath is clinician-in-the-loop AI triage support for oral mucosal lesions. It is designed to help clinical teams review concerning presentations earlier while keeping responsibility and judgement with the clinician.
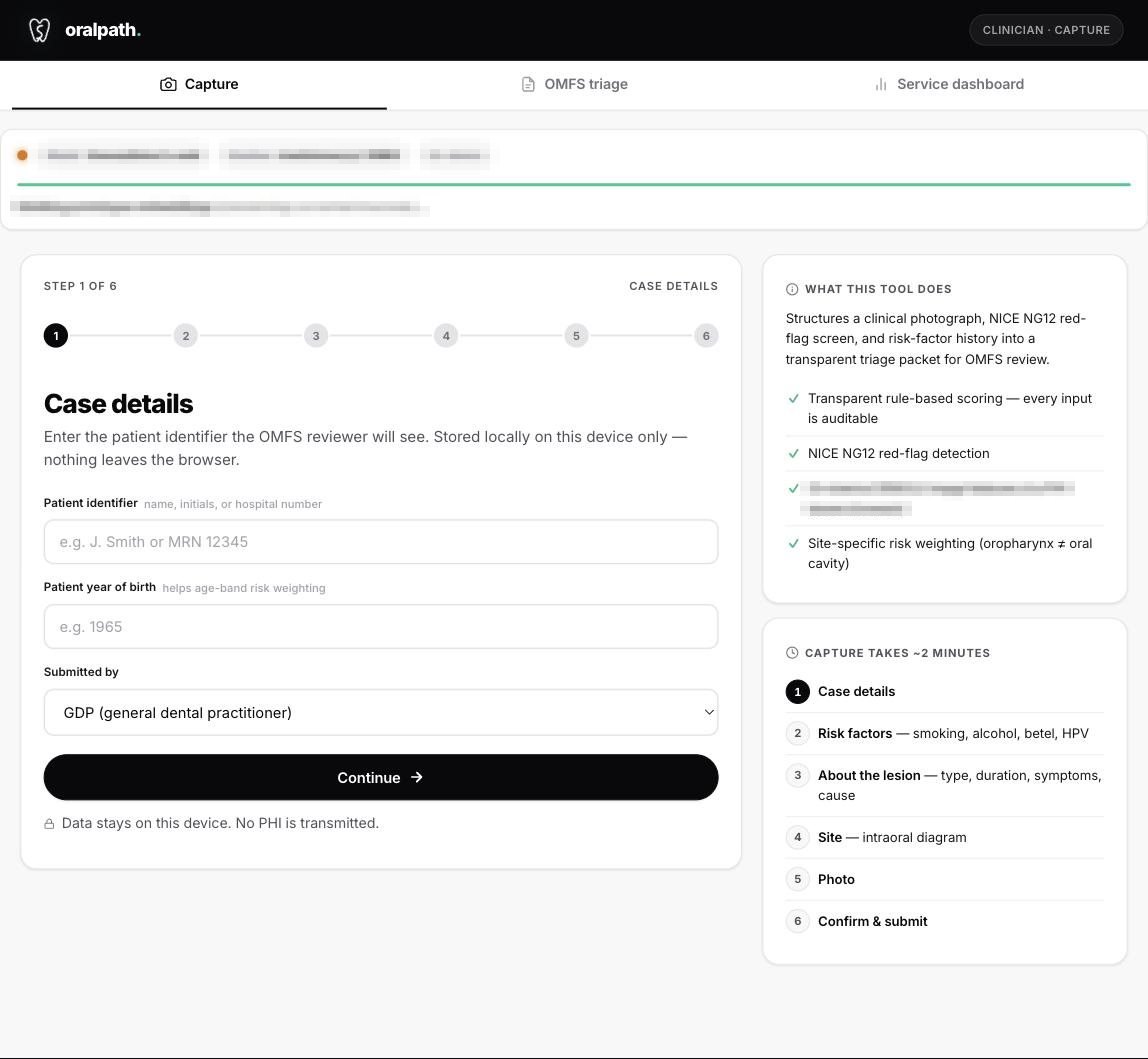
Screens from the live OralPath build. Synthetic sample cohort only — no patient-identifiable information.
OralPath is designed as a clinician-controlled product experience, not a public specification. The page describes the clinical value and safety posture without exposing implementation detail.
Safety boundaries are designed around recognised clinical review expectations without publishing internal logic.
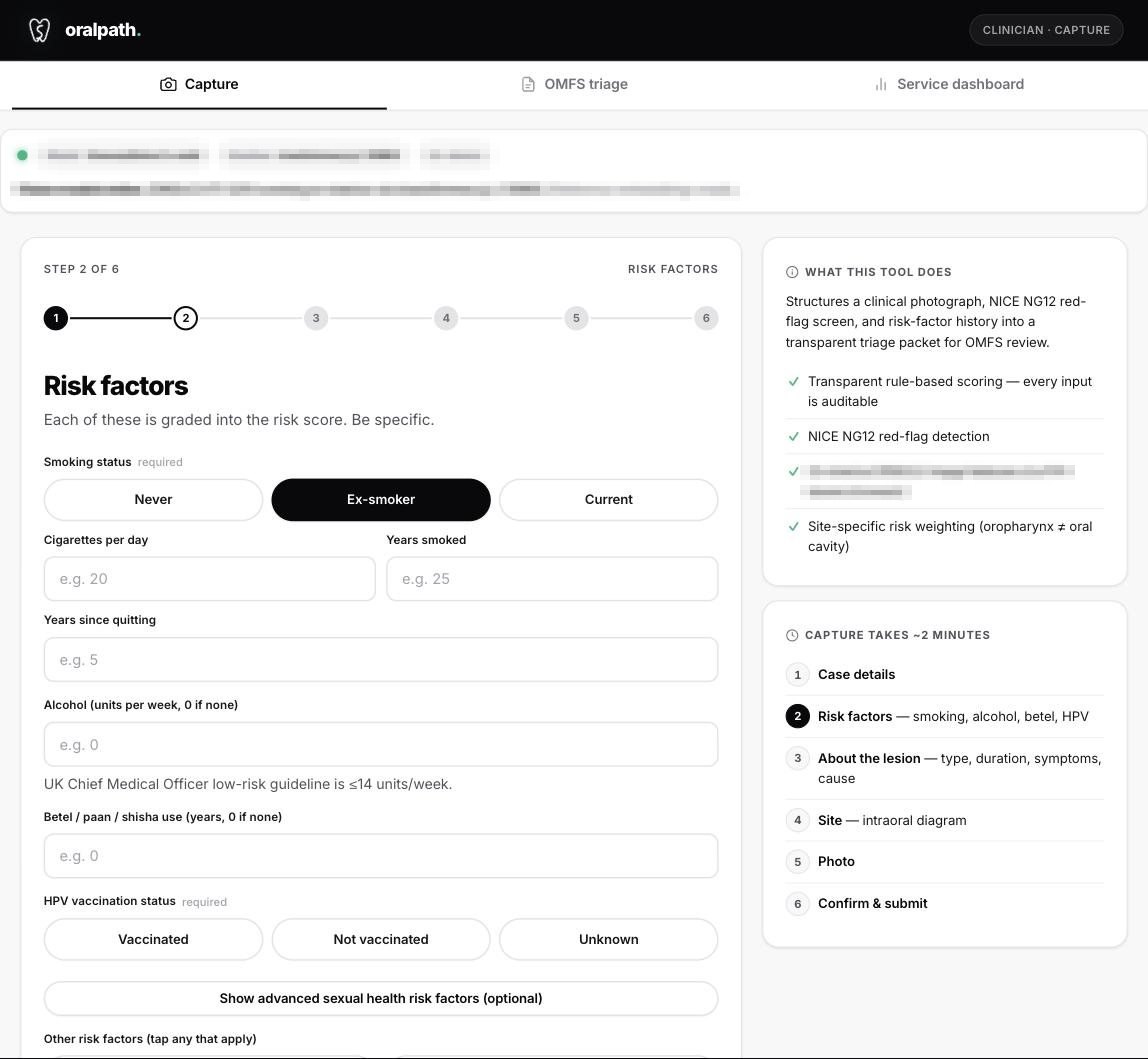
The product experience is designed to reduce variation in how relevant context is gathered and reviewed.
The interface is designed to make the support visible, challengeable and secondary to clinician judgement.
Outputs remain under clinician control, with review and sign-off retained in the clinical workflow.
The public workflow is deliberately high-level. Detailed product behaviour is not published on the open web.
The clinician reviews the presenting context inside a guided product experience.
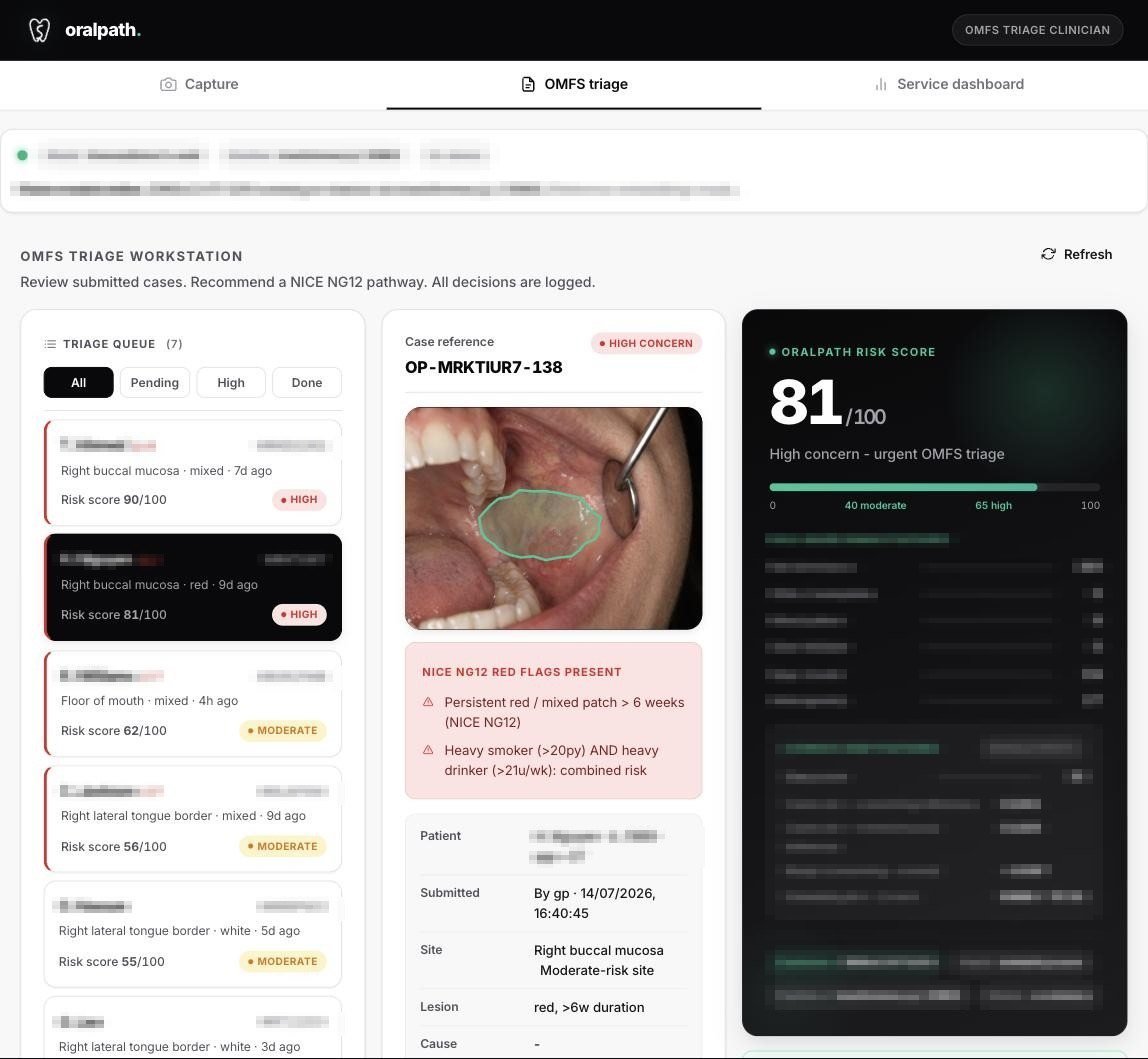
OralPath provides decision-support context without replacing clinical judgement.
Guideline-aware safeguards sit around the product experience.
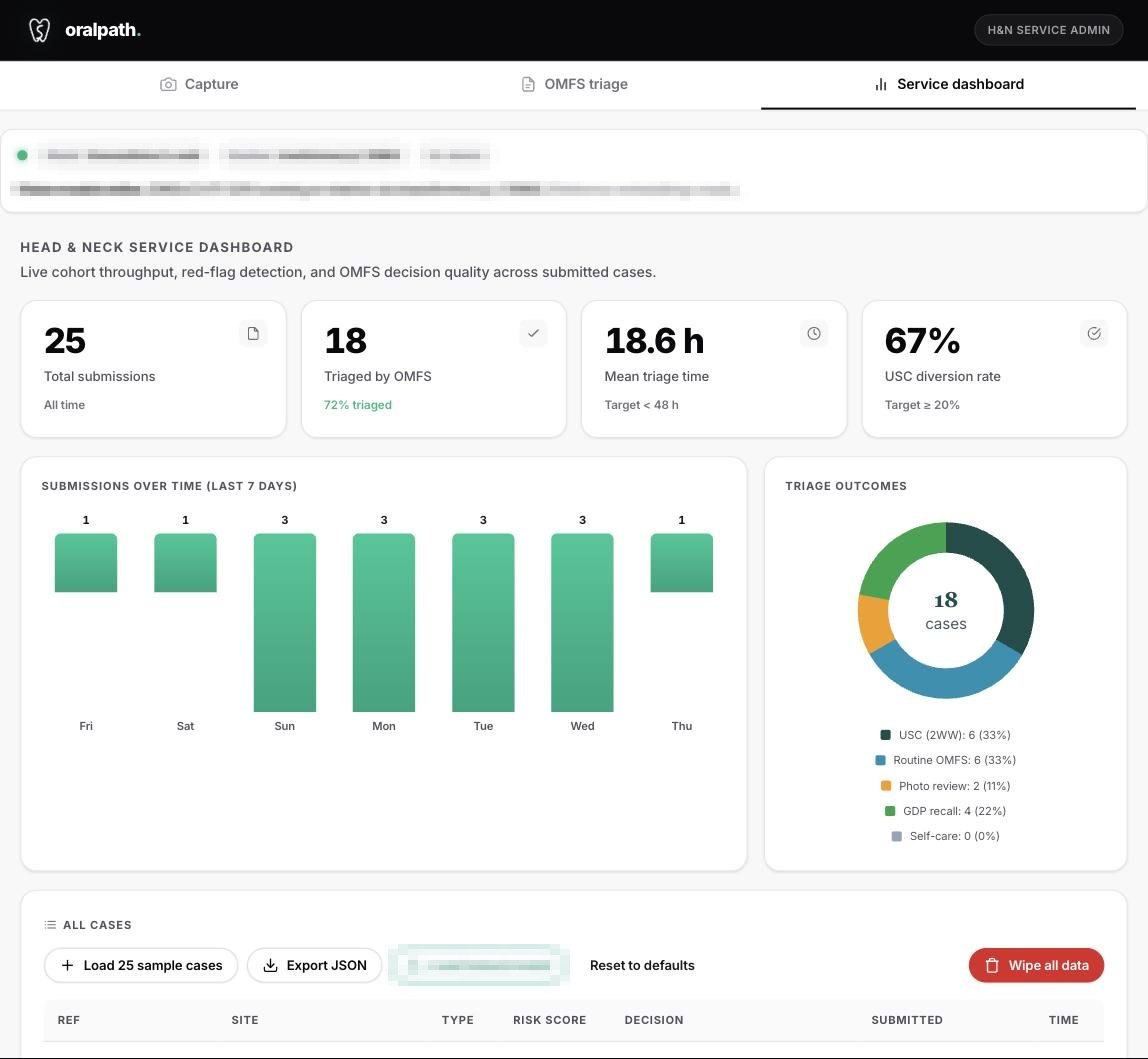
Clinical safety, auditability and deployment evidence are part of the programme.
The responsible clinician remains accountable for the final decision.
OralPath is positioned for clinical triage environments where oral mucosal lesion review needs better structure, safety and governance. Detailed workflow design is shared only with appropriate partners.
Clinical material reviewed in context
Relevant information held together
Guideline-aware safeguards
Clinician review and sign-off
OralPath supports triage review. It does not diagnose oral cancer.
Safety boundaries are part of the product programme, with details reserved for partner contexts.
The responsible clinician reviews the full context and signs the referral decision.
OralPath is built and undergoing clinical validation; safety and performance evidence is published as it reads out (2026/27).
OralPath is available for guided demos with appropriate NHS and dental teams. Public materials intentionally avoid product implementation detail.
OralPath is clinician-in-the-loop AI triage support for oral mucosal lesions. It is built to support safer clinical review without replacing clinician judgement.
No. It is not a diagnosis and does not replace the clinician. It surfaces risk and pathway support for review and sign-off.
No. Public materials describe positioning, safety boundaries and clinical context only. Detailed workflow and implementation details are shared only in appropriate demo or partner contexts.
It is being developed for clinical teams where oral mucosal lesion review needs better structure, safety and auditability.
Request a guided demo through the booking page or email cs@csong.health with your organisation and role. Please do not send patient-identifiable data.
Appropriate clinical teams can review the product in context without public disclosure of product logic or implementation detail.